
There was a report that castration was related to male life expectancy, and menstruation and menopause were related to female life expectancy. First, I examined estrogen, which is a representative of female hormones. Experiments using mice have reported that it has the effect of extending lifespan. I think that the probability that a drug that works on mice will also work on humans is roughly 30%, so you need to be careful when looking at the data. The basis is the results of clinical trials on humans, but as I mentioned before, clinical trials are very expensive, so pharmaceutical companies basically have patents, and they only handle products that have a large number of patients. My stance is to use this 30% supplement or drug that is effective for humans at our own risk based on data from mice. According to an interview article about the administration of sex hormones by Dr. Akishita, professor of geriatrics at the University of Tokyo School of Medicine,
In 1995, the American Heart Association (AHA) commented that estrogen should be administered to all women to prevent heart disease, as it has been reported to suppress arteriosclerosis in humans. The US National Institutes of Health (NIH) conducted a large-scale clinical trial of oral estrogen preparations called the Women’s Health Initiative. However, about five years after the project started, negative data emerged, including increases in myocardial infarction, venous thrombosis, and breast cancer in the treated group, and the project was eventually discontinued. It also resulted in an increase in dementia. Before WHI, about 40% of postmenopausal women in Europe and the United States, and about 20% in Asia, were taking HRT. Currently, each country has its own guidelines for estrogen HRT. In Japan, as a temporary treatment until the body gradually gets used to the sudden change in hormone levels, it is performed with a maximum of 5 years as a guideline for discontinuation. This is because breast cancer increases after 5 years. The estrogen HRT implementation rate in Japan is very low, but in my opinion, it is effective for menopausal and post-menopausal women.
As such, it now appears to be used in a minority of patients for the treatment of menopausal symptoms in women.
Next, I investigated testosterone, the representative of the male sex hormone. In the previous article, I introduced a report that removing all male hormones through castration leads to a longer life, but in reality, various hormones are secreted from the testicles, and testosterone is secreted from the kidney, too. It seems to be more complicated.
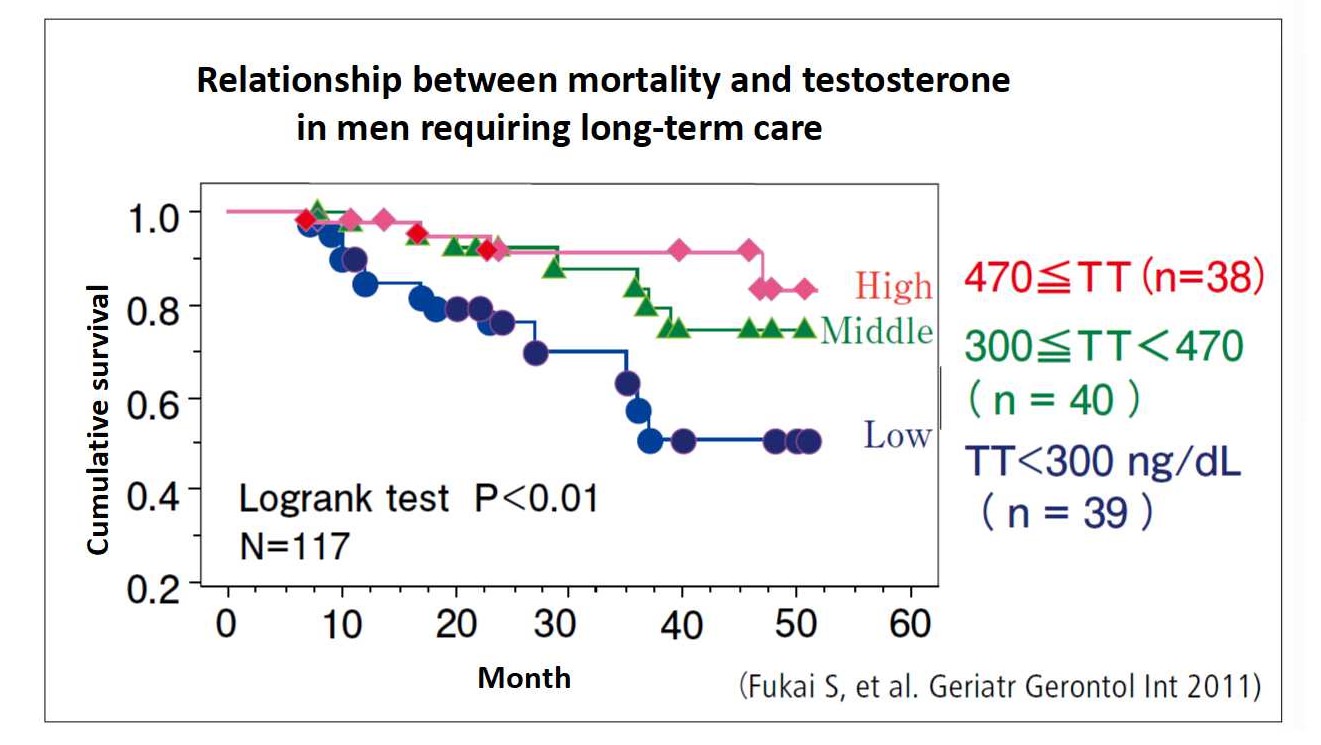
According to “Plasma sex hormone levels and mortality in disabled older men and women” (Fukai S, et al. Geriatr Gerontol Int 2011),
A total of 214 elderly people (117 males and 97 females) aged 70-96 years were followed up. After excluding deaths during the first 6 months, 27 deaths in men and 28 deaths in women occurred during a mean follow up of 32 months and 45 months (up to 52 months), respectively. Mortality rates differed significantly between high and low testosterone tertiles in men, but did not differ significantly between middle and low tertiles. Compared with subjects in the middle and high tertiles, men with testosterone levels in the low tertile (<300 ng/dL) were more likely to die, independent of age, nutritional status, functional status and chronic disease (hazard ratio [HR] = 3.27, 95% confidence interval [CI] = 1.24-12.91). In contrast, the low dehydroepiandrosterone sulfate (DHEA-S) tertile was associated with higher mortality risk in women (multivariate adjusted HR = 4.42, 95% CI = 1.51-12.90). Exclusion of deaths during the first year and cancer deaths had minimal effects on these results. DHEA-S level in men and testosterone and estradiol levels in women were not related to mortality.
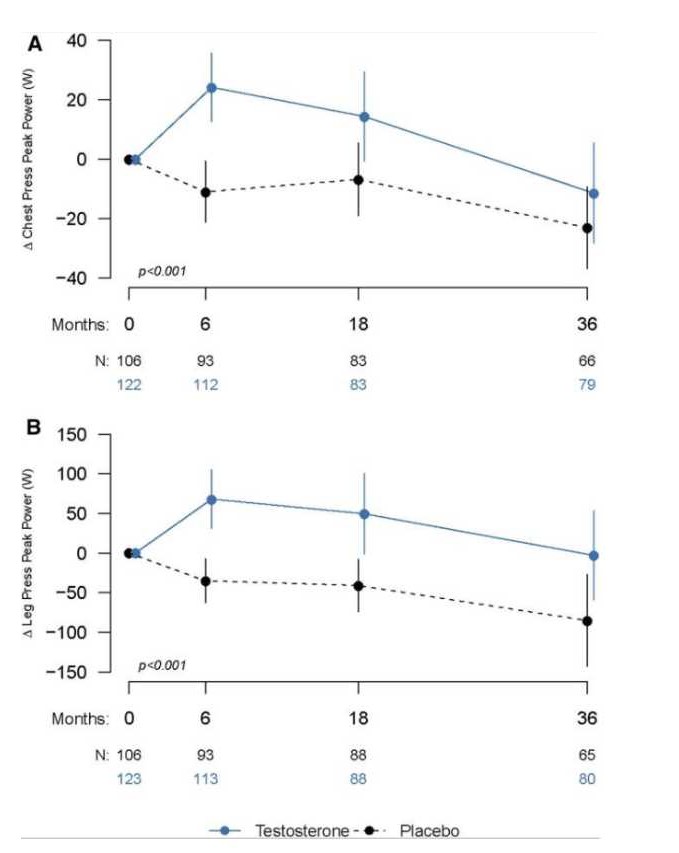 And according to “Effects of Testosterone Supplementation for 3 Years on Muscle Performance and Physical Function in Older Me” (J Clin Endocrinol Metab. 2017 Feb 1; 102(2): 583–593.),
And according to “Effects of Testosterone Supplementation for 3 Years on Muscle Performance and Physical Function in Older Me” (J Clin Endocrinol Metab. 2017 Feb 1; 102(2): 583–593.),
The physical effects of testosterone were investigated in a double-blind controlled trial (N=135 assigned testosterone and N=131 assigned placebo) in healthy men over 60 years of age. The groups were similar at baseline. Testosterone administration for 3 years was associated with significantly greater performance in unloaded and loaded stair-climbing power than placebo (mean estimated between-group difference, 10.7 W [95% confidence interval (CI), −4.0 to 25.5], P = 0.026; and 22.4 W [95% CI, 4.6 to 40.3], P = 0.027), respectively. Changes in chest-press strength (estimated mean difference, 16.3 N; 95% CI, 5.5 to 27.1; P < 0.001) and power (mean difference 22.5 W; 95% CI, 7.5 to 37.5; P < 0.001), and leg-press power were significantly greater in men randomized to testosterone than in those randomized to placebo. Lean body mass significantly increased more in the testosterone group.
Dr. Akishita also said in an interview that both testosterone and DHEA increase with exercise.
A study was conducted in which 12 males with an average age of 66.8 years and potential metabolic syndrome were asked to exercise regularly and observe changes in their bodies. After giving guidance on balance exercise, strength training, and aerobic exercise at the gym twice a month, we observed changes after 3 months of exercising at home five times a week. Here, the waist size did not change, but the average weight decreased by 1 kg, and the visceral fat area decreased by 22%. Blood free testosterone increased from 8.2pg/ml to 9.1pg/ml and DHEA increased by 30%.
In addition, Dr. Akishita said in an interview that testosterone is effective for dementia.
I have investigated the relationship between androgens, cognitive functions, and activities of daily living in a total of 900 elderly people. Some men were given testosterone and some women were given DHEA, and their effects were investigated for six months. Since oral medicines are not available in Japan, we used medicines imported from overseas for the purpose of the survey. In this survey, results such as word memory and delayed playback of whether or not you can remember a while ago have improved. In particular, the effect on testosterone-administered men was remarkable, and I believe that it should be noted that it was at the same level as dementia drugs currently in use, such as Aricept.
DHEA is available as an oral medication, but testosterone is available only as an injection. Currently, there are supplements that promote testosterone synthesis in the body, but I would like to investigate whether they are more effective than exercise. I want to know the side effects and manage them well.
To become good at tennis, you need a certain skill, but how to live longer and rejuvenate requires skill. I would like to provide better information using paid papers, so please donate. You can donate with the coffee icon button
